Definition
Malignant Hyperthermia (MH) is an acute pharmacogenetic (autosomal dominant) disorder, which develops during or immediately after the application of general anaesthesia involving volatile agents and/or depolarising muscle relaxants.
The disorder is as a result of a defect in calcium channel regulation in the muscle cell. Volatile anaesthetic agents and depolarising muscle relaxants interact with the calcium channel resulting in the clinical crisis.
The classic MH crisis is caused primarily by excess calcium availability in the skeletal muscle cytoplasm resulting in excessive muscle contraction and hypermetabolism.
This leads to massive CO2 production, skeletal muscle rigidity, tachyarrhythmias, unstable haemodynamics, respiratory acidosis, cyanosis, hyperkalaemia, lactic acidosis, fever, and eventually (if untreated) death. MH can present with a few or all of these features.
History
Malignant hyperthermia was first described as an entity and noted to be genetically inherited in a letter to the editor of the Lancet in 1960 penned by Michael Denborough and Richard Lovell1 and in a follow up article in 1962 in the British Journal of Anaesthesia2.
The family described showed an autosomal dominant pattern of inheritance for this reaction to anaesthesia. The original letter called for others to share experiences with this type of reaction and the term malignant (“deadly, tending to produce death”) hyperpyrexia (“an abnormally high fever”) was coined.
An excellent summary of the history of MH and anaesthesia3 in Australia has been written by Dr Chris Ball. The article is referenced here and is well worth a read.
A summary of the proposed mechanism of MH
Structural alterations in calcium regulating proteins upset the delicate balance between calcium release from and reuptake into the SR. In normal circumstances (without exposure to volatile anaesthetic agents) in the vast majority of mutations, this balance is maintained. On exposure to volatile agents however, the system is overwhelmed and calcium continues to be released into the cytoplasm beyond the influence of the regulatory proteins.
Restoration of cytoplasmic calcium concentration is paramount to normal cellular function so the reuptake of calcium increases via store operated and excitation contraction coupling. Energy consumption rises dramatically with increased oxygen consumption, CO2 production and heat generation). Muscle gets no chance to relax because of continued calcium exposure (rigidity) and as energy consumption overwhelms oxidative capacity, muscle begins to source energy anaerobically. Lactic acid is produced and the toxic environment of low pH and high Ca2+ that has been created results in cell breakdown and release of creatinine kinase.
Differential Diagnosis
This is one of the more challenging differential diagnoses because time to treat is critical.
If in doubt consider that:
- Dantrolene is a safe drug with the provision of appropriate ventilatory support
- Extreme hyperthermia can result in cell death and an unsalvageable situation
- Not all symptoms of MH need to be present to make the diagnosis
If you have inappropriate tachycardia, elevated CO2 and hyper or hypotension, rapidly exclude:
- Insufficient anaesthesia
- Insufficient ventilation or gas flow
- Saturated soda lime
- Machine malfunction
- CO2 from laparoscopic insufflation (note MH has occurred in laparoscopic cases)
If there is ongoing masseter spasm or rigidity and the situation is stable it may be worth considering the response to the addition of non-depolarising muscle relaxant?
- Masseter spasm and rigidity related to MH should not resolve with a non-depolarising muscle relaxant
Also consider the following differentials:
- Phaeochromocytoma – extreme fluctuations in arterial blood pressure, hyperthermia, sweating, usually no muscle involvement
- Infection, septicaemia – hyperthermia, usually no muscle involvement
- Thyroid Storm –hyperthermia, no rigidity but may have rhabdomyolysis
- Central anticholinergic syndrome – delayed emergence, hyperthermia and nystagmus, dilated pupils
- Serotonergic syndrome – Triggering agent (serotonergic, cocaine, MDMA, ketamine, methylene blue and SSRI), no nystagmus
- Neuroleptic malignant syndrome – slow onset hyperthermia (24-72 hours after withdrawal of dopamine agonist)
- Mismatched blood transfusion, blood in the fourth cerebral ventricle, drug toxicity and drug allergies may cause isolated hyperthermia
Masseter Spasm
True masseter spasm can be the first and sometimes only sign of MH. True masseter spasm is a prolonged, palpable tightening of the masseter muscles that does not release gradually. The difficulty is usually distinguishing this from an inadequate dose of suxamethonium and the normal increased tone seen with suxamethonium in some patients.
There are two approaches to the patient with true masseter spasm
- Discontinue volatile anaesthesia, continue the case with total intravenous anaesthesia and watch for signs of MH. Treat accordingly if signs develop. Refer to an MH diagnostic centre for follow up.
- Abandon surgery and treat for MH if any other signs develop. Refer to an MH diagnostic centre for follow up.
The decision to take either of the above approaches may be influenced by the following realities:
- Testing for MH is not usually performed in patients who are less than 30kg or under ten years of age
- Testing will not be performed for at least three months after an episode of masseter spasm
- Patients need to travel to a testing centre for the biopsy
Disorders Associated with MH
Patients with central core disease (CCD) and multiminicore disease (MMD) with gain of function RYR1 defects are at risk of MH. While those with CCD and MMD and a loss of function RYR1 defect should not be at risk of MH, this may not be clear based on symptomatology or genetic testing. The safest position is to treat all CCD and MMD patients as potentially MH susceptible unless they have had a negative IVCT. CCD and MMD are often asymptomatic in childhood.
King-Denborough syndrome is a myopathy with an RYR1 defect and patients should be considered at risk for MH.
Patients who have a history of exertional heat illness (EHI) with no obvious predisposing factors may be at increased risk of MH. This is more likely of they have had repeated episodes in temperate climate and if there is a familial component to the EHI.
A myopathy caused by a defect in the STAC3 gene manifest as muscle weakness with cleft palate known as “Native American myopathy” is also associated with MH.
The In vitro contracture test (IVCT)
All current Australian and New Zealand laboratories follow the guidelines of the European Malignant Hyperthermia Group.
The EMHG guidelines are summarised as follows:
- The minimum patient age for the muscle biopsy is 4yr, but laboratories should not test children younger than 10yr of age without relevant control data. Laboratories may also set minimum body weight limits
- The minimum weight limit for Australian and New Zealand laboratories is 30kg
- The minimum age for IVCT is 10 years
- The biopsy should be performed on the quadriceps muscle (either vastus medialis or vastus lateralis), using local (avoiding local anaesthetic infiltration of muscle tissue), regional, or trigger-free general anaesthetic techniques.
- The muscle samples can be dissected in vivo or removed as a block for dissection in the laboratory within 15 minutes
- The time from biopsy to completion of the tests should not exceed 5 hours
- Muscle specimens should measure 20-25mm in length and at least four tests should be performed each one using a fresh specimen
- The tests should include a static cumulative caffeine test and a dynamic or static halothane test. The results should be reported as the threshold concentration, which is the lowest concentration of caffeine or halothane that produces a sustained increase of at least 2mN (0.2grams) in baseline force from the lowest force reached.
- The laboratory diagnostic classification includes:
- MHShc: a caffeine threshold of 2mmol/litre or less in at least one caffeine test and a halothane threshold concentration of 0.44 mmol/litre or less in at least one halothane test.
- MHSh: a halothane threshold concentration of 0.44 mmol/litre or less in at least one halothane test and a caffeine threshold of 3mmol/litre or more in all caffeine tests.
- MHSc: a caffeine threshold of 2mmol/litre or less in at least one caffeine test and a halothane threshold concentration above 0.44 mmol/litre in all halothane tests.
- MHN: a caffeine threshold at a caffeine concentration of 3mmol/litre or more in all caffeine tests and a halothane threshold concentration above 0.44 mmol/litre in all halothane tests.
- MHShc, MSHh and MHSc are all considered to be susceptible to MH
- Laboratory MHN diagnosis is good evidence that the patient is not at risk of developing MH. An MHN-tested individual cannot transmit MH risk to their offspring
Molecular genetic detection of susceptibility to malignant hyperthermia
All current Australian and New Zealand laboratories follow the guidelines of the European Malignant Hyperthermia Group (EMHG).
The EMHG guidelines are summarised as follows:
Predictive testing based on a known familial mutation
- If an MH-associated RYR1 mutation has been identified in the index case, the RYR1 mutation can be used for predictive testing of relatives.
- Persons carrying the familial mutation should be regarded as MH susceptible
- Persons who do not carry the familial mutation cannot be regarded as completely risk free (in about 5% of large pedigree studies there is discordance between IVCT results and genetic data) and should such persons seek maximal safety, an IVCT should be considered.
RYR1 mutation screening as a diagnostic test
- A clear clinical indication is a prerequisite for any genetic testing
- Genetic testing can be performed as a targeted analysis of known associated MH mutations or as screening of entire coding regions
- If one of the known MH mutations is identified, the person should be considered at risk of MH
- As yet unclassified sequence variants will frequently be identified using entire coding region sequencing. The MH laboratory is responsible for checking the available published evidence and for applying prediction algorithms with the aim of eventually classifying the variant as neutral or potentially MH associated
- For patient safety, individuals carrying a ‘potentially MH-associated’ RYR1 variant should be regarded as at increased risk for MH until further diagnostic tests (i.e. an IVCT) have been performed
Clinical Malignant Hyperthermia
Signs of an MH Crisis
Early Signs
- Prolonged masseter muscle spasm after suxamethonium
- Inappropriately raised end tidal carbon dioxide during controlled ventilation or tachypnoea during spontaneous respiration
- Inappropriate tachycardia
- Cardiac arrhythmias; particularly ventricular ectopic beats
Developing signs
- Rapid rise in temperature (0.5°C per 15 minutes)
- Progressive metabolic and respiratory acidosis (ABG)
- Hyperkalaemia
- Profuse sweating
- Cardiovascular Instability
- Decreased SpO2 or mottling of skin
- Generalised muscular rigidity
Later signs and symptoms
- ‘Cola’ coloured urine – due to myoglobinuria
- Generalised muscle ache
- Grossly raised serum CK
- Coagulopathy
- Cardiac arrest
In Brandom’s 20104 paper which examined 268 AMRA (adverse metabolic and or musculoskeletal response to anaesthesia) reports the most frequent initial MH signs were hypercarbia, sinus tachycardia, or masseter spasm, however; temperature abnormalities were also a relatively early sign.
Treatment of an MH crisis
Immediate management with intravenous dantrolene is essential as is stopping the trigger agent.
Therefore:
- Give dantrolene as a priority
- Turn off volatile agent and hyperventilate with very high flows (15L/min) of 100% O2. Do not waste time changing the circuit or the anaesthetic machine
- Declare an emergency and where possible stop the surgery
- Commence non-triggering anaesthesia (TIVA)
Dantrolene
Dantrolene 2.5mg/kg total body weight (not lean body weight) IV – initial push and repeat as necessary
- Dosing is the same per kg for paediatric patients
- Mobilise other sources of dantrolene (you may need at least 36 ampoules)
- Mix each ampoule with 60mls sterile water
- Dantrolene can be given peripherally or centrally
Simultaneously treat the life-threatening events:
Hyperkalaemia
- Hyperventilate and treat the acidosis
- CaCI2 10%(0.15ml/kg = 10mls = 7mmol in adults)
- Insulin 0.15u/kg + dextrose 50% 0.5ml/kg (10u + 50ml in adults)
Hyperthermia
- Cool the patient if T > 38.5°C
- IV normal saline at 4°C: surface cooling with ice
- Consider peritoneal lavage with normal saline at 4°C if the peritoneum is already accessed
Acidosis
- Hyperventilate to at least normocapnia
- Consider sodium bicarbonate 0.5 mmol/kg IV as necessary to maintain pH >7.2
Arrhythmias
- Lignocaine 1-2mg/kg
- Amiodarone 2-3mg/kg over 15 minutes
- Consider hyperkalaemia as a cause of rhythm disturbance
Additional Monitoring
- core temperature
- arterial blood pressure (arterial line)
- Urine output via catheter (aim for >2ml/kg/hr)
- Central venous access and monitoring
Pathology Tests
- Send urgent bloods and repeat frequently to monitor success of therapy
- ABG
- U+E
- FBC
- CK
- COAG
- Myoglobin (serum and urine)
When the patient is stabilised:
- Admit for close monitoring in an intensive care environment
- Monitor the patient for at least 24hrs post reaction
- Recurrence may occur and large amounts of dantrolene may be needed in the first 24 hrs
- Consider mobilising additional sources of dantrolene
- Consider transferring patients with fulminant reactions to major centres after stabilisation
Post-operative MH5
Postoperative MH is uncommon occurring in less than 2% of cases. All cases of post-operative MH (as reported in AMRA registry) occurred within 40 minutes of cessation of triggering agent.
Postoperative MH has been reported in the anaesthetic literature. A careful evaluation of these published cases reveals that they seem to follow one of four clinical patterns:
- Classic acute MH occurring shortly after the completion of surgery and the general anaesthetic
- Atypical MH manifesting as delayed rhabdomyolysis in patients subsequently identified as MH susceptible by contracture testing
- Unsubstantiated reports made doubtful by the absence of positive contracture testing or unconvincing clinical characteristics
- Cases in which the initial presenting signs of MH seemed to begin in the intraoperative period
Classic MH with an initial presentation in the postoperative period is rarely reported; in addition to the cases found in the North American Malignant Hyperthermia Registry (NAMHR), only three additional published reports were identified.10–12 The clinical characteristics of these patients resembled the AMRA cohort of cases with regard to presenting signs and the short latency time of onset after the completion of the general anaesthetic. Of note, none of the published cases presented with hyperthermia without additional signs of acute MH.
Postoperative rhabdomyolysis in patients with proven MH susceptibility is more common. In all reported cases, the initial presentation was the onset of brownish discoloration of the urine, which then prompted further evaluation and discovery of rhabdomyolysis. Classic signs of MH such as generalized rigidity, tachypnoea, tachycardia, and hyperthermia were absent. It is presently unclear whether patients who present with post-operative rhabdomyolysis and subsequently demonstrate an abnormal caffeine–halothane contracture test result have an MH-causing mutation, or a subclinical muscle disease which results in a false-positive contracture test result.
Preparing for the MHS patient
Patients with one of the following should be considered potentially susceptible:
- Previous malignant hyperthermia reaction as yet untested
- Positive in vitro contracture test (IVCT) on muscle biopsy
- Positive DNA test for MH
- Relative has positive IVCT and patient has not had an IVCT
- Patient (with MHS relative) has negative DNA result
- Relative with clinical MH reaction and patient has not had an IVCT
Preparation of a Boyle’s anaesthesia machine (or equivalent)
Remove vapouriser; replace soda-lime with fresh soda-lime. Replace hoses and rebreathing bags with new hoses and bags. Flush with 10 L/min oxygen or medical air for at least 20 minutes (at least 30 minutes if isoflurane has been used recently in the anaesthetic machine) through the circuit using a new rebreathing bag as an artificial lung, including the ventilator and carbon dioxide absorber in the circuit.
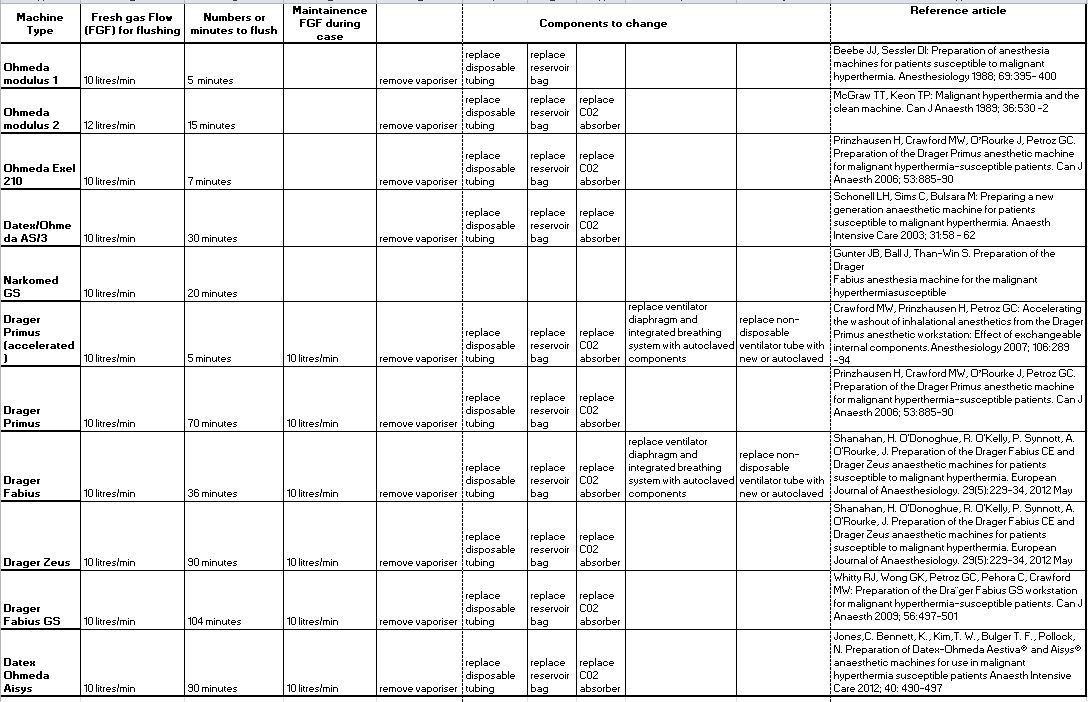
Anaesthesia Workstation preparation
Different workstations may require longer times for flushing. See the table below for your workstation. If your machine is not present on this list you may have to consult the appropriate peer reviewed publication for more information or contact the manufacturer.
Charcoal filters may be effective alternatives to long flush times. See the MHANZ statement on charcoal filters here.
General principles for all anaesthetic workstations after appropriate flushing are:
- Use a new mask, new LMA or new ETT
- Continue to use HIGH FLOWS throughout the anaesthetic to avoid accumulation of small quantities of volatile agent
- Preferably place MHS patients first on the operating list
Monitoring
- During surgery monitor and record temperature and respiratory rate in addition to standard ANZCA guidelines (PS18)
- After surgery continue minimum mandatory monitoring as per PS4 (Charcoal Filter Article – ANZCA Bulletin March 2014)
- All patients should have a temperature recorded on arrival and on leaving PACU
- There is no requirement to keep patients in PACU for longer than for standard patient care
Drugs that MUST be avoided with MHS patients
- Depolarising muscle relaxants (i.e. suxamethonium)
- ALL potent inhalational agents – including; desflurane, sevoflurane, isoflurane, enflurane, halothane, methoxyflurane
Drugs that can be used with MHS patients
All other pharmacological agents are safe including the following common drugs:
- Nitrous oxide (and xenon)
- Propofol and all intravenous induction agents including ketamine and benzodiazepines
- Non-depolarising muscle relaxants
- Local anaesthetics with or without adrenaline
- Opioids and other analgesics,
- Syntocinon, ergometrine, magnesium sulphate,
- Ephedrine, metaraminol, phenylephrine
Patients with a negative in vitro contracture test can receive normal anaesthesia
1 Denborough M, Lovell, RR. Anaesthetic deaths in a family. Lancet 1960; 2: 45
2 Denborough MA, Forster JF, Lovell RR, Maplestone PA, Villiers JD. Anaesthetic deaths in a family. Br J Anaesth 1962; 34: 395-6
3 Ball C. Unravelling the mystery of malignant hyperthermia. Anaesth Intensive Care 2007; 35 Suppl 1: 26-31
4 Larach MG, Gronert GA, Allen GC, Brandom BW, Lehman EB. Clinical presentation, treatment, and complications of malignant hyperthermia in North America from 1987 to 2006. Anesth Analg 2010; 110: 498-507
5 Litman RS, Flood CD, Kaplan RF, Kim YL, Tobin JR. Postoperative malignant hyperthermia: an analysis of cases from the North American Malignant Hyperthermia Registry. Anesthesiology 2008; 109: 825-9
Begin the Competency Test
Simply click on the link below to begin the multiple choice competency test.