MH is a potentially life-threatening condition which is avoidable if anaesthesia is given with no triggering agents.
Some MH susceptible individuals present outside of the operating theatre. Known associations with MH susceptibility are exertional rhabdomyolysis, hyperCKaemia, exertional heat illness, central core disease and multiminicore myopathy. There are also rare reports of MH susceptible individuals who present with episodes of fever and muscle rigidity unrelated to drug exposure that can prove fatal.
The British Malignant Hyperthermia Association website states that:
“MH susceptibility was originally described as an autosomal dominant condition with incomplete penetrance. There is mounting evidence that MH susceptibility is one of a growing number of presumed single gene disorders that deviates from a simple Mendelian model of inheritance. Indeed, inheritance of MH can be best explained by a threshold model: approximately 8% of UK MH families appear to have more than one genetic factor making a major contribution to the risk of MH susceptibility.”
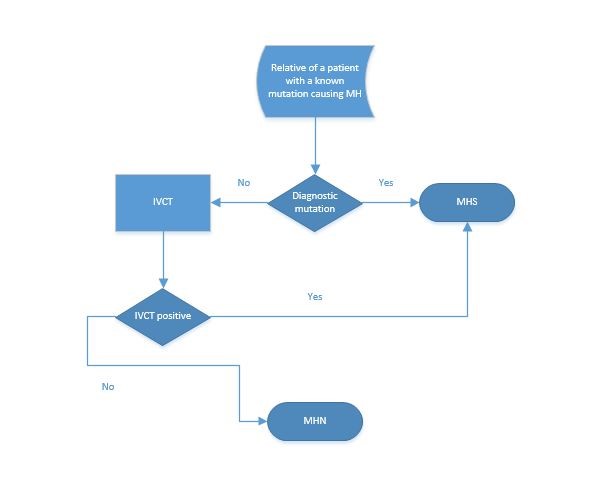
MHANZ member laboratories (all of whom follow the EMHG testing guidelines) offer an in-vitro contracture test (IVCT) to family members who test negative for the family mutation.
MHANZ is conservative with interpreting predictive genetic tests. MHANZ recognises many families that have discordance between genotype and phenotype suggesting the presence of a second mutation or a modifying variant.
As a result genetic diagnosis of MH with the presence of a known causative mutation is possible but the converse is not true.
The only way to rule out MH is with a biopsy, absence of the family mutation isn’t good enough.
Many RYR1 variants have been found in MH and non-MH susceptible individuals. Currently the EMHG assigns causality to variants that meet the following criteria:
- A minor allele frequency of less than 1%
- Functional characterisation in an approved system 1
Pathogenicity predictors such as ….. are not helpful in determining RYR1 variant functionality
In most cases MHANZ laboratories will test a person who has had a possible MH episode with an In Vitro Contracture test and then continue to RYR1 and CACNA1s testing once the diagnosis is confirmed. In some cases genetic testing is appropriate as a first diagnostic step.
Ideally, genetic testing for MH should be done in consultation with an MH diagnostic unit (link to contact details of MH units in Aust and NZ)- please provide.
1 Hopkins PM RH, Snoeck MM, Girard T, Glahn KPE, Ellis FR, Müller CR, Urwyler A on behalf of the European Malignant Hyperthermia Group. The European Malignant Hyperthermia Group guidelines for the investigation of malignant hyperthermia susceptibility. Br J Anaesth 2015; 115: 531-9